There is an argument out there that acupuncture can do great good, but does not harm people if incorrectly used. On a number of boards I have argued that incorrect use or choice of points can cause harm or even death. I am not talking about needling into the skull or an unclosed fontanel for children, but use of the regular channel points. I think in the West, there is sometimes a cavalier approach to acupuncture, that we can use certain points and it “will always be ok.”
In my own experience, I have had a practitioner needle Lung 5 on me, when I had no apparent respiratory distress or cough. I was perfectly healthy and receiving a “tune up.” I woke up the next day with my left lung filled with fluid, breathing felt like it was being done under water. I went back to the student-practitioner and she didn’t know what the reason was for the breathing issue, but that maybe I had “caught bronchitis over night.” This was not malpractice, simply a student who had not been taught to not needle certain points in certain situations. While in acupuncture school, I found that for the most part the contraindications for needling that I was taught had more to do with the structure of the body, rather then the Chinese diagnosis. It is apparent from reading the classics that the diagnosis is just as important when it comes to picking which points NOT to needle.
I am a practicing acupuncturist, and I don’t say these things to breed fear, but to raise awareness that being attentive to our choice of points – must be the norm.
Wáng Zhízhòng 王執中 in his Zhēn Jiǔ Zī Shēng Jīng 針灸資生經 (The Classic of Supplementing Life with Acupuncture and Moxibustion) translation by Dr. Yue Lu (forthcoming) said:
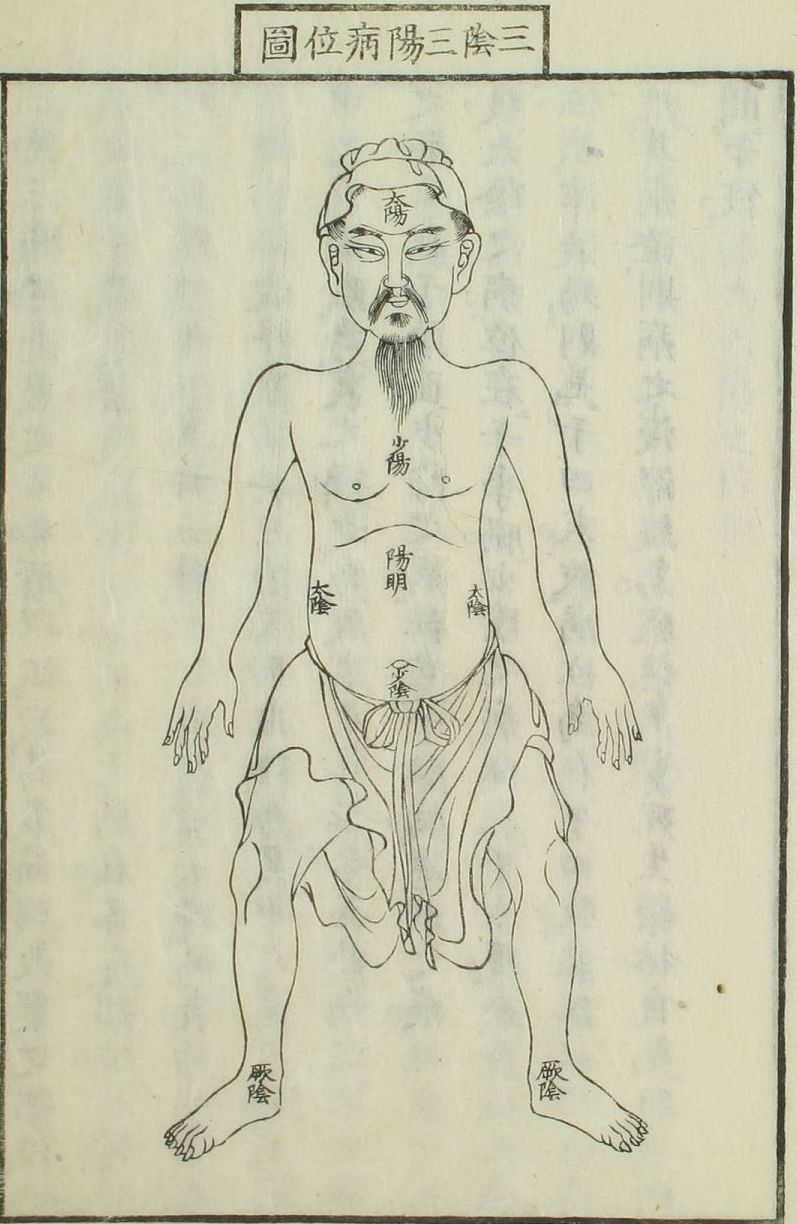
“水腫惟得針水溝,若針余穴,水盡即死,此《明堂》、《銅人》所戒也。庸醫多為人針水分,殺人多矣。若其它穴,亦有針得瘥者,特幸焉耳,不可為法也。
Only needle Shuǐ Gōu 水溝 (Dū 26) for edema; if other points are needled, people will die after water becomes exhausted. This is the contraindication from Míng Táng 《明堂》 and Tóng Rén 《銅人》. Vulgar healers usually needle Shuǐ Fēn 水分 (Rèn 9) on patients, so they have killed a lot of people. If other points are needled, it will be very lucky for these people to recover afterwards. This cannot be set as the standard principle.”
The classics were clear the improper use of acupuncture could cause great problems. Wáng Zhízhòng is also clear that there are “vulgar” healers, who are essentially lay people with only a limited amount of training. You see where this goes: when seeing any other practitioner who practices acupuncture, but has not gone through enough training, there are risks. By seeing a practitioner of Chinese medicine who is cavalier about their point choices, there are risks.
I could go on, but that takes us into political agendas and scholastic reform, neither of which I have the qi to move forward on right now 😉 So practitioners, here is a good reminder to be attentive with your choice of points. Patients: be attentive about your choice of practitioners.